×
![]()
Caroline Giroux MD

Image courtesy: Caroline Giroux
Being a physician is often about exploring and listening to stories. The life of a healer is full of stories. The ones heard, the ones fantasized, the ones forgotten, the ones re-emerging in dreams. As physicians, we become part of them by listening to the words the patient says, but also to the symptoms of each malady, those symptoms that are the words of the body. Storytelling is one of the four pillars of meaning; it is a universal need and also a healing force. But there is another aspect to it: as a physician, I do believe that storylistening brings joy and meaning to our work. Richard Mollica said that by listening, you become part of the story (Mollica, 2008). You bear witness to the traumas that have happened to the person who shares a story.
You can expect to do a lot of that throughout your medical career. Yet, it is important to stay in touch with your own need to tell stories. To find your own narrative and see how it is woven with each patient’s narrative crossing paths with you. For some of your patients, you must know that you will be the only human being they will encounter the day of their medical appointment. You might even mean the world to them. The gift of their stories and trust is a precious one. You can give back by letting patients impact you.
As a physician, you have the opportunity to do both storylistening and storytelling, as you simmer in powerful and inspiring stories. This is a captivating journey that will continue beyond our medical training years if you let yourself embrace your patients’ vulnerabilities and your own. Being vulnerable means being authentic, human and courageous, and the field of medicine needs the authentic, human, and the brave presence that you already are.
When we sit in front of a patient and conduct an assessment, the data-gathering process will be unique in the sense that no one will take the same steps or enter the same doors - the patient’s statements - to further the exploration. It becomes a co-construction between the interviewer and the interviewee. Each patient’s story becomes a foreign land even though some elements sound familiar. We can go from disbelief to stupor, from horror to awe. The awe is usually what keeps us going, what makes us wanting to continue to work in the trenches of medicine, including human psyche. Despite all the potential depletion the role of physicians entails, there is an amazing source of replenishment and growth that occurs as well, in our patients and in those whose role is to support them. We might have the feelings we live vicariously through our patients, witnessing their strides and feeling the pains and the joys as if they were our own. We may suffer as if the evil had been done to us, too. The unfolding of their lives can go in various directions and be a proxy for our own meaning to life; a vicarious living, full of vicarious wounds, but also full of creative possibilities.
The expression vicarious trauma can be confusing and ambiguous, especially because trauma implies an experience of toxic stress, which is what people seek to avoid, yet people tend to use "vicarious trauma" and "secondary trauma" (or secondary traumatic stress) interchangeably. However, vicarious trauma is not necessarily a bad thing and it can be transformative, as opposed to "secondary traumatic stress," which can encompass posttraumatic stress disorder (PTSD) symptomatology in the person close to or working with survivors of trauma (National Center for PTSD). (See section Know Yourself, topic Compassion Fatigue, Vicarious Trauma, and Burnout on definitions.) An expression that is more and more frequently used in the wellness vernacular is vicarious resilience, which is more positive terminology and probably a more fitting expression. Once the trauma has occurred in a patient, whether we have secondary traumatization from hearing about it or not, we can all benefit from vicarious resilience (e.g., indirectly experiencing the patient’s own resilience through some kind of mirror-neuron process, or our own that is boosted from hearing a story resonating with our past or connecting us to the suffering of the whole of humanity). It can be a general process taking place through time, after having heard many patients’ stories, or it can occur after one powerful therapeutic process with a particular patient. In order to access that ability to bounce back, people have usually some innate resilience factors such as dispositional mindfulness, interpersonal support or self-care tools (see toolkit and other self-care strategies elsewhere in this e-learning tool), which in turn make it easier for the clinician to see the positive in most stressful experiences.
In summary, vicarious resilience is about:
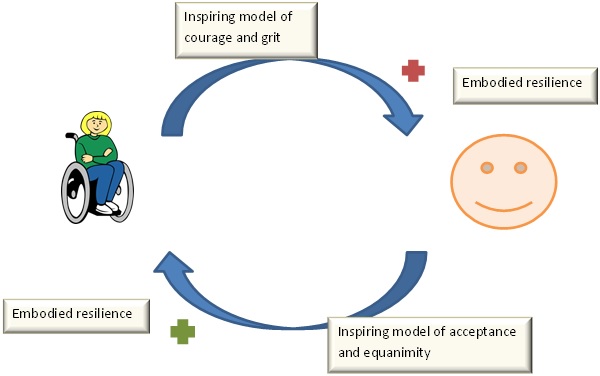
Figure 1. Vicarious resilience feedback loop between patient and clinician
People are inspired by stories of women, men, and children who have triumphed over adversity or injustice. Please complete the resilience buidling exercise below.
| Which books did you read as a child or adolescent that made a strong impression on you? | Which movie character(s) would you like to resemble? |
|---|---|
For example, the author of this topic has found the following books to be inspirational to her.
| Write a short narrative explaining why, or a thank-you letter to this patient for having expanded your perspective. |
|---|
We, physicians, have one of the most captivating, mythical, and romanticized jobs. We hear stories. We act as healers. But often we feel trapped in our own emotional responses. How to resolve this? How to gain strength and resilience to continue to work effectively with wounded patients and make a difference? We create an interaction or “life scenario”, a new, more adaptive script with the patient, for the patient. We view each patient as co-director because they have inner strengths that can break the shackles of their trauma.
Using the framework of vicarious resilience in medicine means progressing, transforming, from being the spectator to actor to director. Ultimately, we should aim to become not only spectators of others’ lives, or actors from one life to the other, but director of our own life dynamics, oscillating between the three states when appropriate to context instead of when forced to do so by triggers or malevolent forces.
Being the spectator is an essential role in certain interactions (e.g., when someone needs a compassionate ear). It can be a neutral, comfortable or uncomfortable experience, none of which is a bad thing as long as it is transient and tolerable. However, being forced to be a voiceless, helpless spectator, or feeling trapped in the victim role (as in traumatic experiences) can be disempowering, and moving towards the two subsequent stages described below will help healing.

Image credit: pixabay
Most people feel in control when they go about their lives with the persona they think they have more or less chosen (e.g., physician, teacher, spouse, parent, daughter, son). With such roles in society usually come specific and often implicit scripts or sets of rules that maintain the balance within a complex system. Yet, under duress a solid actor can lose that balance and experience distress, emotional paralysis and, hence, feel more like a spectator. It is important to develop awareness of changing roles and scripts throughout the lifespan to adapt to developmental challenges and move towards a more integrative, transcending step, such as sitting in the movie director’s chair.

Image credit: pixabay
As opposed to the actor being told what to do, the director is like a conductor and aims at integrating various levels of contributions to ensure a cohesive, harmonious performance. The movie director keeps the global picture in mind and wants to maximize everyone’s contribution to attain a broader goal. At times, the spectator of the actors is asked to give them feedback and, at times, the actor tends to model self-development and a thriving existence and, thus, the director will have a versatile role that integrates the trauma story in the overall life narrative. Working behind the scenes allows to see the whole forest instead of just a few trees and integrate various perspectives. The stage of ego transcendence makes it easier for the director to no longer crave admiration from being frequently on stage. The director acts like a coach and draws satisfaction from his team’s work and performance; he/she seeks individual and collective growth. The director’s ultimate goal is to ensure everyone in the troop develops the ability to sit in the director’s chair to co-direct trauma-centred therapy, work-family balance, and general life goals.

Image credit: pixabay
Table 1 summarizes the three stages of empowerment using the performance arts analogy.
| Spectator | Actor | Director |
|---|---|---|
| Observer | Emotional and behavioural enacting | Multiple perspectives |
| Passive | More active, but conforms to the director’s and spectators ideas/expectations | Integrative, all-encompassing Empowering, transcending |
| Role: “Trauma victim” (direct experience) |
Role: “Trauma survivor” working towards healing or trauma therapist (direct/indirect) |
Role: Empowered person who is reconnecting with inner self and resilience factors (more indirect, detached; more mindfulness leads to less overidentification with the victim role) |
| Acute survival, numbness | Chronic survival mode, fight or flight, “survival of the fittest” at risk of re-victimization | Awareness, lives rather than survives |
| Direct trauma | Secondary traumatization | Vicarious “success” or resilience (rejoices in the cast’s performance) |
 Victims of trauma are often helpless spectators witnessing, in shock, parts of their selves being neglected, violated, and abused. At some point, the actor engages in an acting role through narration and efforts in healing. Once the person can transcend the spectator’s and actor’s part of a bigger script, he/she becomes the director of the theater of his/her own life, producing resilience and emanating empowerment. Who wants to join our medical field and help spectators become enlightened and inspiring movie directors?
Victims of trauma are often helpless spectators witnessing, in shock, parts of their selves being neglected, violated, and abused. At some point, the actor engages in an acting role through narration and efforts in healing. Once the person can transcend the spectator’s and actor’s part of a bigger script, he/she becomes the director of the theater of his/her own life, producing resilience and emanating empowerment. Who wants to join our medical field and help spectators become enlightened and inspiring movie directors?