×
![]()
Tara Riddell MD
Burnout is by no means a new concept. In fact, the term was first coined back in 1974, by psychologist Herbert Freudenberger, when he published a paper on the matter in the Journal of Social Issues. In his essay, Freudenberger (1974) reviewed how he and his fellow colleagues, who had been tirelessly working in a free clinic, began to experience a state of “burnout,” in which they became physically, mentally, and emotionally worn down. Though it was thought to affect anyone, even at that time Freudenberger highlighted that it was “the dedicated and the committed” who were prone to burnout, particularly those who were in caregiving roles, and who worked serving the community, especially in the fields of social services and healthcare (Freudenberger, 1974).
Shortly thereafter, Maslach identified the three dimensions of burnout (emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment) (Maslach et al, 1981). Though burnout itself is believed to have a vast array of symptoms, these manifestations have been largely accepted as the core of the burnout syndrome and have been heavily featured and utilized in the development of burnout assessments, such as the Maslach Burnout Inventory; a screening tool which has even been adapted for those working in medicine and is considered the gold standard in research literature (Thomas, 2004).
Since then, the field of literature around burnout has exploded, as evidenced by 159 million and over 3.5 million results emerging from a simple Google search on “burnout” and “physician burnout” respectively. There’s no doubt that burnout exists and affects a large proportion of medical learners and physicians; however, even despite this knowledge, without proper awareness, it can go unrecognized. For example, in a 2017 study of burnout among emergency medicine residents, 30 trainees completed a burnout assessment and their faculty advisors were privately surveyed and asked to predict whether their residents were experiencing burnout or not. Though 70% of residents were found to be experiencing burnout, only 17% were identified by the faculty advisors, suggesting that prediction and identification of resident burnout was quite poor (Lu et al, 2017).
Though data is still lacking on how well trainees and physicians can identify burnout amongst themselves, this suggests that education and building awareness on how to recognize burnout and its manifestations is a crucial first step in both prevention and management endeavours.
Amanda is a 28-year-old first year obstetrics/gynecology resident. She recently graduated from medical school, which was a huge accomplishment, as not only did she reach one of her dreams, but she became the first in her family to become a physician. Though she enjoyed medical school and made several lifelong friends, she constantly was pushing herself so that she would not just succeed, but excel. Amanda was her own toughest critic, but all the time, effort, and sacrifices paid off when she graduated with distinction and matched to her first choice residency program.
In the summer following graduation, Amanda married her partner Adam, who works as an accountant. As her residency program was located in another city, the pair prepared for a new adventure together and packed up their lives, moving a few days’ drive away from their families. When her first day rolled around, Amanda felt a little nervous, but was buoyed by her excitement to start this new chapter.
Several months later, Amanda is nearing the end of her first year. She is currently on her internal medicine rotation, which she has found demanding, given the call frequency and the fact that she has always personally found internal medicine to be somewhat challenging. Despite this, her staff and seniors have been supportive and encouraging, which has helped build her confidence, and she has felt satisfied in her clinical work, helping to care for and treat various patients.
Similar to many new residents, Amanda also applied in her first year to complete one of the requisite medical licensing exams, which is now upcoming in the next few weeks. While Amanda has slowly been studying for this over the past little while, in the month prior to the exam, Amanda begins to fret. Due to her work and call schedule she has not been able to meet regularly with her study group or stay on track with her studying. She is no longer sure that she will be able to cover and review all the material she needs to and as such, she worries about being unprepared come exam day, which may lead to failure. Amanda feels overwhelmed, and wonders how she will get through this.
To make this a little clearer, let’s consider these concepts on somewhat of a continuum (see Figure 1).
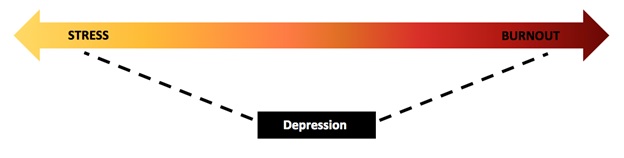
Figure 1. The continuum between stress and burnout
Whether trying to complete a research grant or manuscript by a specific deadline, studying for board exams while continuing clinical duties as a resident as in this case, or having a patient crash in the middle of the night while on call, we can all attest to times when we felt stressed, particularly within our workplace.
Similar to these examples, we experience stress when the demands and pressures pile up, leading us to feel anxious and overwhelmed, because it seems like too much and things in that moment feel out of our control. Our bodies also react, as even with a psychological stressor, the HPA-axis is activated and epinephrine is released kick-starting the fight or flight response and putting us into overdrive. As a result, we feel a sense of urgency, our emotions are heightened, and though we may feel tired, we increase our engagement and activity to try to cope, and avert danger or failure.
Metaphorically then, stress is akin to being hit by wave, which pulls us out to sea. We feel overwhelmed and as though we are drowning, but we can still see the shore and know if we paddle hard, we might just be able to get back to land and safety.
When stress becomes persistent and unremitting however, this can set the stage for burnout (Kumar et al, 2005). As with stress, we are still overextended, facing increased demands and responsibilities; however, this continually depletes our resources and energy, until we feel empty and have nothing left to give. In the wake of this, exhaustion sets in, we become negative and detached due to having lost sight of our utility and purpose, and we feel incompetent and unproductive, leading to decreased motivation, helplessness, and decreased engagement.
To help conceptualize this, Dike Drummond, a family physician and the founder of TheHappyMD.com, suggests imagining a bank account that symbolizes our emotional, physical, and spiritual reserves. When well, we make withdrawals from this account, such as to function in our roles at home and at work, but we also make deposits to maintain a positive balance, whether through a good night’s sleep, seeing our friends, or feeling fulfilled from our job. However, when experiencing burnout, we make more withdrawals and less deposits, and as such eventually we go into the negative. When in the red, with no reserve left, it makes it immensely hard to give to others and to function optimally (Drummond, 2015).
Though depressive episodes can occur without any clear stressors or precipitants, signified by the placement of depression outside the continuum in Figure 1, it is known that stressful life events can certainly be a risk factor for depression (American Psychiatric Association, 2013). In addition, emerging evidence suggests there is an association that exists between burnout and depression.
Given Freudenberger’s statement that those with burnout “look, act, and seem depressed” and the apparent overlap with regards to symptomatology, some have questioned whether burnout and depression are in fact separate entities. However, one key distinction revolves around the area of one’s life that is impacted. Burnout for instance is considered a “distinct work-related syndrome” (Wurm et al, 2016), whereas depression tends to be more widespread and permeates multiple dimensions of an individual’s life (Shanafelt et al, 2003).
In addition, Brenninkmeyer et al (2001) suggest that there are other distinguishing features between these two concepts. They specifically suggest that those with burnout tend to:
While there is still a lack of longitudinal and prospective data to better understand the precise relationship between burnout and depression, it is suspected that there is a bidirectional relationship, and particularly that untreated burnout can lead to depression and suicide. This makes sense, as if burnout persists, sapping all your energy and time, this could subsequently impact your roles and functioning in other areas.
Though Amanda had gone through a stressful period while preparing for her licensing exam, requiring her to manage her time more wisely, and focus her studies to the topics she was less familiar with, she successfully completed the exam, and the remainder of her first year rotations. When second year began, Amanda felt more relaxed and was excited to focus more exclusively on her medical specialty (obstetrics/gynecology).
A year and a half later, Amanda is now in the midst of her third year of residency. Since starting residency she has received great evaluations from her preceptors and has become comfortable with managing cases independently, particularly when in on-call situations. In addition to her clinical rotations, Amanda has taken on some extra roles including acting as a social chair for her specialty residents’ council, the teaching of medical students, and in working on a research project in sexual medicine.
At night, Amanda has been having trouble falling asleep, as she tends to run through all that is on her ever-growing to-do list, and has difficulty turning off her mind and relaxing. As such, she has been having a harder time getting out of bed in the morning, as she feels tired and exhausted, which persists throughout the day.
Though Amanda had chosen obstetrics and gynecology due to her interest in pursuing a career in the subfield of sexual medicine for her passion of learning and exploring an individual’s story and has been well-liked and respected by her patients given her empathic nature and the time she devotes to encounters, Amanda has been feeling like she is just running through the motions. She caught herself recently listing off questions robotically during follow-up visits, with less interest in her patients, such that the validation and feedback she reflexively provided didn’t always feel entirely genuine. On a few occasions she even realized she hadn’t been paying much attention to the patient and wasn’t actively listening. She has found herself particularly troubled by some of her patients whom she has been following closely, as either they fail to engage in treatment leading her to feel frustrated or irritable, or they fail to get better which leads her to feel defeated and as if nothing she does is helpful. She has found that she is less confident and decisive when formulating a management plan, and has begun to doubt her own skills and knowledge, feeling as though she is not keeping up with her co-residents.
Though she has still been making an effort to spend some of her free time with her friends and spouse, she has not had the time to visit the gym in ages, which used to be an enjoyable outlet for her, as she has been tirelessly trying to tackle all of her responsibilities. In addition, now more often than not, whenever Amanda has some spare time at home, due to her fatigue, she often is finding herself drawn to her couch and TV. She has also been finding that her neck and back are quite tense and stiff, and she has been having more frequent migraines, which have led to her needing to take her first sick day in her medical career.
| Physical | Emotional | Mental/Cognitive |
|---|---|---|
| Insomnia | Anger or irritability | Trouble focusing |
| Fatigue | Cynicism or pessimism | Forgetful, indecisive |
| Headache | Overwhelmed, anxious | Decreased motivation |
| Changes to appetite | Apathetic or detached | Procrastinating or avoiding |
| GI upset | Sad, depressed | Slower to complete tasks |
| Aches, pains and tension | Self-doubt | |
| Increased illness | Decreased self-esteem |
Table 1 shows a summary of the signs and symptoms of burnout, but you can learn more about each feature of burnout by clicking on the icons below.



Now that we have had a chance to learn more about what it means to be burned out, it is time to check-in with yourself to see if you may be exhibiting any warning signs and to evaluate your current level of wellness.
To assist with this, visit one of these sites which offer free, confidential, and quick (less than 5 minute) assessments of workplace distress, burnout, and wellness specifically for physicians:
Consider Amanda’s case as described previously.
Though there are no definitive diagnostic criteria for burnout, in research an individual is often considered to be burned out if they have at least one of the three manifestations, particularly if they score highly within the realms of exhaustion or depersonalization. Amanda demonstrates signs and symptoms from all three categories, which strongly suggests that she is burned out.
See explanation at statement YES.
Fatigue
Disrupted sleep
Disrupted appetite
Somatic symptoms
Trouble concentrating
Indecisive
Overwhelmed
Cynical
Irritable
Detached and impassive
Sad or depressed
Reduced productivity
Feeling incompetent
Doubt abilities and skills
Lost sense of meaning or purpose in work
As the weeks pass, Amanda continues to struggle. Though she senses she is burning out, she hopes that if she continues to push through and tackle some of the projects on her plate, then maybe things will take a turn for the better. However, her fatigue and exhaustion continue to make being productive challenging, and the demands never seem to lessen.
Amanda continues to feel overwhelmed and is distressed by the fact that she is not living up to her high standards and expectations. She begins to second guess her clinical decisions, and worries about making a mistake, particularly after she had forgotten to book a patient’s follow-up appointment in her calendar causing a disgruntled patient, stressed administrative staff, and her busy preceptor being forced to help cover for her, when the patient arrived seemingly unannounced.
In addition, on call one night when working with a pregnant patient with a comorbid diagnosis of borderline personality disorder, though Amanda had felt that they had developed a fairly good alliance initially, when the patient engaged in splitting and refused to partake in decision-making around treatments being offered, Amanda became more terse and irritable. This resulted in the patient leaving angry and refusing all care, leading Amanda to feel poorly about herself and her skills, and questioning her value and purpose.
Amanda continues to feel more and more behind in her work and studies. She even missed a deadline for a draft of her research paper, which greatly bothered her as she used to pride herself on her organization and time management. She continues to try and keep up; however, in doing so her work-life balance, which was tenuous to begin with, begins to crumble as she spends less time with her family and friends, and is often noted to decline social engagements.
At home, things are also falling by the wayside as Amanda has little energy to engage in housekeeping, and as such her home often appears in disarray, adding more angst. She and her husband have been getting into more arguments, as Amanda tends to come home frustrated and irritable, with little patience. When home, Amanda has also been having 1-2 glasses of wine, which is a change for her, having previously only drank on the weekends.
Amanda’s mood gradually declines, along with her motivation. She notices that she doesn’t enjoy her work or even her hobbies as much, and getting out of bed and getting ready in the morning is a chore. As she has not been exercising and has been eating more lately, Amanda notices she has gained some weight, which also further injures her self-esteem. Whether at home or at work, Amanda perpetually feels as if she’s letting down those around her, which causes significant guilt. Lately at night, she’s been feeling hopeless and on a few occasions she has had fleeting thoughts that maybe everything would be better if she wasn’t around.
As in our case, burnout if left untreated can have significant impacts in various ways, including on our own wellbeing, our professional development, and the care we provide to patients. Table 2 shows a summary of the impacts of burnout.
| Personal | Professional |
|---|---|
| Motor vehicle accidents | Less empathy |
| Impaired personal relationships | Medical errors |
| Substance abuse | Suboptimal patient care |
| Depression | Unprofessional behaviours |
| Suicidal ideation | Reduced medical knowledge / performance |
| Career dissatisfaction and turnover |
3 Regarding burnout consequences (see Table 2), take the True/False Quiz below.
In a 5-year prospective cohort study of internal medicine residents by West et al in 2012, over 50% of residents reported a motor vehicle incident (either a crash or near miss). Those who reported burnout, lower quality of life, or who screened positive for depression, were at significantly higher risk.
While we do not have a lot of research yet that explores the risk of burnout with other accidents/injuries, we do know that those with burnout are often fatigued and that many physicians are sleep deprived especially if they work on-call. Sleep deprivation in itself can pose a significant risk to our own wellbeing, particularly as our performance tends to be impaired similar to if we had been drinking with a BAC of 0.04-0.05% or higher (Philibert, 2005; Williamson & Foyer, 2000). In addition, a study of residents found that those who slept less than 5 hours a night were 1.8 times more likely to have a serious accident or injury, such as due to needlestick injury or with a motor vehicle accident (Baldwin et al, 2004).
Many articles on burnout often cite marital discord as a consequence of burnout. A study of over 500 American physicians similarly demonstrated a strong association between burnout and both impaired relationships with family members as well as difficulty maintaining friendships outside of medicine (Campbell et al, 2001).
See statement at section True.
While there is a lack of data regarding physicians’ use and abuse of recreational or certain prescription drugs, several studies support an association between burnout and risky alcohol use among both medical learners and physicians (Jackson et al, 2016; Pedersen et al, 2016). For example, in a study of over 7,000 U.S. physicians, a strong association was found between burnout, depression, suicidal ideation, and reduced quality of life or career satisfaction with alcohol abuse and dependence.
See statement at section True.
Though it is difficult to determine causation, many studies do suggest that burnout is highly associated with mental health conditions, such as depression and anxiety (Pereira-Lima et al, 2015). In addition, in one study, when compared to physicians unaffected with burnout, those with burnout were at higher risk of suffering from major depression. This risk of depression was also found to be directly related to the severity of burnout, as the odds of having depression was three times more likely for those with mild burnout compared to those without, 10 times more likely for those with moderate burnout, and 93 times more likely for those with severe burnout (Wurm et al, 2016).
See statement at section True.
A study of over 4,000 medical students found that burnout was a predictor for suicidal ideation, such that students were two to three times more likely to report suicidal ideation if they were experiencing burnout (Dyrbye et al, 2008). This study also showed that recovery from burnout significantly decreased the rates of suicidal ideation, suggesting that suicidal ideation could potentially be reversed (Dyrbye et al, 2008).
See statement at section True.
Studies have shown that among physicians from various specialties there is a negative correlation between burnout and one’s level of empathy (Walocha et al, 2013). In addition, a study of 400 Canadian psychiatry residents found that those with burnout were more likely to feel that their capacity for empathy in clinical situations was impaired or compromised (Kealy et al, 2016). Altruism can also be impacted as a study of over 2,000 medical students found that students with burnout were significantly less likely to hold altruistic views about a physician’s responsibility to society and one’s community, particularly those who are underserved or marginalized (Dyrbye et al, 2010).
See statement at section True.
While it is difficult to monitor and study true errors among physicians, an association between burnout and rates of self-perceived medical errors has been found (West et al, 2006). In a study of pediatrics residents, residents who were burned out were significantly more likely to report having made a significant error and reported a higher number of errors in the preceding month, although there was no objective evidence of increased errors. Residents who were depressed, however, made six times as many medication errors as their non-depressed co-residents, and were more likely to report having worked on a few occasions in an impaired condition (Fahrenkopf et al, 2008).
See statement at section True.
For example, a study of 115 residents found that residents who were burned out were 2-3 times more likely to self-report engaging in poor patient care or attitudes (i.e., failing to properly discuss treatment options or fully answer a patient’s questions, discharging a patient to make the team more manageable, having little reaction to the death of a patient) at least monthly or weekly (Shanafelt et al, 2002).
See statement at section True.
The literature does suggest that burnout can impair the development of important professional skills, such as honesty and integrity, which can also have negative repercussions on delivery and quality of patient healthcare (Dyrbye et al, 2016). For example, a multi-site study of medical students demonstrated that students who were experiencing burnout or depression were more likely to engage in unprofessional behaviours, such as cheating during an exam, reporting that a physical exam finding was normal when it had not been assessed, or reporting that they had ordered a test when this was inaccurate (Dyrbye et al, 2010).
See statement at section True.
Data suggests that burnout can negatively impact cognitive function and performance. For example, in one study, a small group of residents underwent fMRI while being asked multiple choice medical questions. They found that those with burnout had changes to their cognitive functioning, specifically, there was reduced activity in the dorsolateral prefrontal cortex and right middle frontal gyrus, which suggests that both empathy and clinical reasoning can be impacted (Durning et al, 2013). Further, in a U.S. study of over 16,000 internal medicine residents, those with burnout scored significantly lower on a national standardized medical exam compared to those without. In addition, the differences in scores on the exam seen across the severity of burnout were as large as the differences seen between different years of training (West et al, 2011).
See statement at section True.
Regardless of the profession, studies have shown that employees who are burned out tend to experience higher job dissatisfaction, which can lead to absenteeism and eventually leaving their work creating more turnover (Brown et al, 2009; Felton, 1998). The same holds true for physicians, as those with burnout tend to be more dissatisfied with their work-life balance (Shanafelt et al, 2012), and data does support a negative association between burnout and job satisfaction (Xiao et al, 2014). In addition, in a study of over 2,000 medical students, those with burnout were more likely to have serious thoughts of dropping out.
See statement at section True.